Are you losing up to 15% of anesthesia revenue each year due to preventable billing errors? Anesthesia billing is unlike that of other medical specialties. It is uniquely unit‑based, time‑dependent, and modifier‑sensitive, making accuracy and efficiency critical for practice revenue. According to recent industry data:
- 12–18% of anesthesia claims are denied on first submission, significantly higher than the average physician service claim denial rate of 5–10%.
- Practices can lose 8–15% of annual anesthesia revenue due to billing inefficiencies, coding errors, or documentation gaps.
- Manual processes contribute to nearly 40% of claim delays or denials, highlighting the impact of workflow inefficiencies on financial performance.
These figures make it clear that anesthesia billing is far more than a documentation task. It is a strategic financial lever that affects cash flow, operational efficiency, and the long-term sustainability of healthcare practices. Practices that leverage AI-driven coding, automated workflows, and proactive denial management consistently outperform peers in revenue recovery and claim accuracy.
What Is Anesthesia Billing and Coding?
Anesthesia billing and coding involve accurately translating clinical anesthesia services into billable claims using standardized codes, detailed documentation, and precise time tracking.
Unlike procedural specialties that bill by service, anesthesia reimbursement is calculated using a multi‑factor unit system reflecting:
- Base units (procedure complexity)
- Time units (actual anesthesia care duration)
- Provider role modifiers
- Patient physical status modifiers
This complexity increases the risk of underpayment or denials if even one element is inaccurate. According to a 2025 MGMA survey, practices with optimized anesthesia billing workflows reported up to 22% fewer denials and 15–20% faster reimbursements compared to practices without structured coding processes.
Core Components of Anesthesia Billing Units
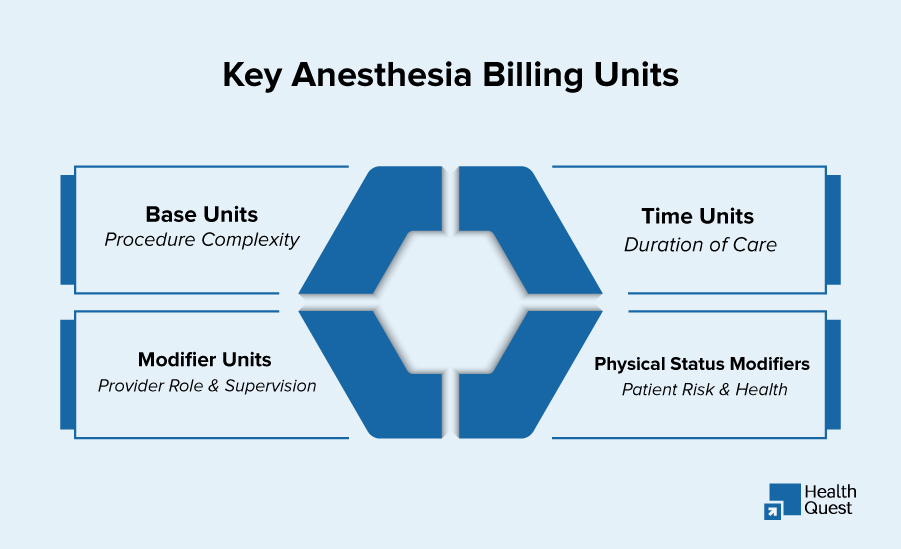
Anesthesia billing relies on a combination of base units, time units, and modifier units. Understanding each component is critical for accurate reimbursement, minimizing denials, and optimizing revenue. Below, we break down these core elements in detail.
-
Base Units: Procedure Complexity
Base units reflect the intrinsic complexity of an anesthesia service and are determined using ASA (American Society of Anesthesiologists) guidelines. They account for the technical difficulty, risk, and intensity of the procedure.
Examples:
- Minor procedures → Low base units
- Complex surgeries → Higher base units
Historical ASA data show that base units range from 1–19 per procedure, depending on surgical complexity. Accurate assignment of base units ensures appropriate reimbursement and prevents underbilling.
-
Time Units: Duration of Anesthesia Care
Time units are calculated based on the actual duration of anesthesia care, typically 1 unit per 15 minutes. These units include pre-operative preparation, intra-operative management, and post-operative emergence.
Key Industry Benchmarks:
- Average anesthesia procedures last 90–120 minutes, translating to 6–8 time units.
- Practices with poor time tracking can underbill by 5–8% annually.
- Even a 10-minute error in documenting induction or emergence can result in lost revenue or audit exposure.
Precise time tracking is essential for compliance and maximizing reimbursement.
-
Modifier Units: Provider Role and Supervision
Modifier units indicate the provider’s role in anesthesia delivery, influencing reimbursement levels. They clarify whether services were personally performed or medically directed, and whether CRNAs were involved.
Common Modifiers:
- AA – Anesthesiologist personally performed the service
- QK – Medical direction of 2–4 CRNAs
- QX – CRNA with medical direction
- QY – Medical direction of one CRNA
Improper use of anesthesiologist and CRNA modifiers is a leading cause of claim denials, accounting for approximately 15–20% of coding-related issues. Proper application ensures accurate reimbursement and reduces compliance risks.
-
Physical Status Modifiers (P1–P6)
Physical status modifiers reflect the patient’s overall health and medical risk during anesthesia. They are critical for accurately capturing the complexity of care and justifying appropriate reimbursement.
Modifier Breakdown:
- P1 – Healthy patient
- P2 – Patient with mild systemic disease
- P3–P6 – Patients with progressively severe conditions, including emergencies or severe systemic disease
These modifiers are essential because higher-risk patients require additional resources, monitoring, and attention, which can increase total billing units. Proper documentation of physical status modifiers ensures compliance, reduces denials, and supports fair reimbursement for complex cases.
How to Calculate Total Anesthesia Billing Units
Understanding anesthesia billing units is only useful if you know how to combine them accurately. Total billing units determine the final reimbursement and are calculated using a simple formula:
Total Units = Base Units + Time Units + Modifier Units + Physical Status Modifiers
Step-by-Step Calculation
- Start with Base Units
Base units reflect the complexity of the procedure. For example, a minor outpatient procedure may have 3 base units, while a major surgery may have 10–15 units according to ASA guidelines. - Add Time Units
Time units are based on anesthesia care duration, typically 1 unit per 15 minutes. For instance, a 90-minute procedure adds 6 time units. - Include Modifier Units
Modifier units depend on the type of provider involvement:- AA – Anesthesiologist personally performed the service
- QK – Medical direction of 2–4 CRNAs
Correct usage is crucial, as improper modifiers can result in 15–20% of coding-related denials.
- Apply Physical Status Modifiers
Add units for patient risk factors (P1–P6). Higher-risk patients justify additional reimbursement due to increased complexity and resource needs.
Example Calculation
- Base Units: 8 (complex surgery)
- Time Units: 6 (90-minute procedure)
- Modifier Units: 1 (medical direction)
- Physical Status Modifier: 2 (P3 patient)
Total Units = 8 + 6 + 1 + 2 = 17 units
Revenue Implication:
At an average anesthesia conversion factor of $22 per unit, this procedure would generate $374. Even small errors in unit calculation can result in significant revenue loss across multiple procedures.
Common Anesthesia Billing Mistakes and How to Avoid Them
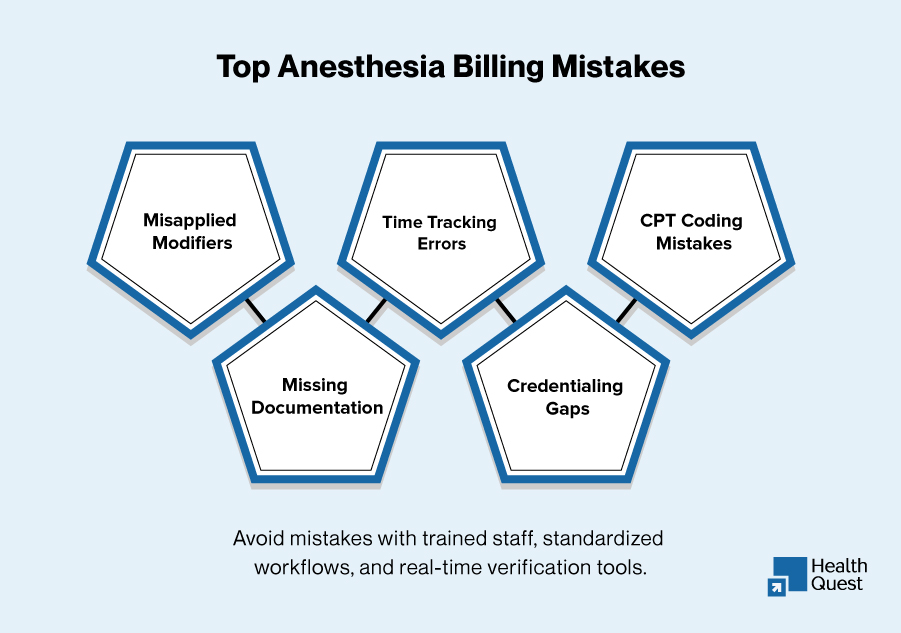
Even small errors in anesthesia billing can cost practices thousands in lost revenue. The most frequent pitfalls? Misapplied AA, QK, QX, or QY modifiers, inaccurate start and end times, incorrect CPT codes, missing physical status or CRNA documentation, and gaps in provider credentialing or payer enrollment.
Avoiding these mistakes isn’t just about checking boxes; it’s about creating a system that works. Practices that invest in trained billing staff, standardized workflows, and real-time verification tools catch errors before claims are submitted, reduce denials, and protect every dollar of revenue. In 2026, precision in billing isn’t optional; it’s a financial necessity.
Top Challenges Threatening Anesthesia Revenue in 2026
Anesthesia billing is inherently complex, and practices face multiple hurdles that can directly impact revenue, compliance, and operational efficiency. Understanding these challenges is critical for minimizing claim denials and maximizing reimbursement.
-
Complex Coding Requirements
Anesthesia billing requires precise coding for every procedure, modifier, and time unit. Unlike general physician billing, each anesthesia service is unit-based and sensitive to factors such as procedure complexity, patient status, and provider supervision. Misapplied codes, incorrect units, or missing modifiers are major contributors to denied claims. Industry data shows that 12–18% of anesthesia claims are denied on first submission, nearly double the average physician claim denial rate. Keeping staff trained on ASA guidelines, CPT updates, and payer-specific rules is essential to maintain accurate billing and avoid revenue leakage.
-
Time Tracking Errors
Time units form the backbone of anesthesia billing, yet tracking pre-op, intra-op, and post-op times accurately remains a common challenge. Errors in recording start and end times, even by a few minutes, can result in underbilling, lost revenue, or audit exposure. Studies indicate that practices with poor time tracking can underbill by 5–8% annually, highlighting the critical importance of precise documentation and automated time-tracking tools.
-
Credentialing and Provider Enrollment Gaps
Billing errors are not limited to codes and units; administrative gaps, such as incomplete provider credentialing or inactive payer enrollment, can cause claims to be denied outright. Claims submitted under non-credentialed or unregistered providers are almost always rejected, leading to delayed payments and increased administrative burden. Maintaining up-to-date records in CAQH, NPPES, and payer portals, along with monitoring license expirations, DEA registrations, and board certifications, is essential to avoid these costly delays.
-
Denied Claims and Rework
Even with accurate coding, denied claims are a common obstacle. Payers may reject claims due to documentation gaps, missing authorizations, or misapplied modifiers. Handling denials consumes significant staff time and can create cash flow disruptions. Industry reports show that manual processes contribute to nearly 40% of anesthesia claim delays or denials. Implementing a thorough review process before submission, coupled with automated alerts and denial-tracking workflows, can reduce rework and accelerate reimbursement.
-
Regulatory and Coding Updates
Annual updates in CPT codes, ASA guidelines, and payer-specific policies introduce another layer of complexity. New procedures, changes in base units, and revised modifiers can significantly impact reimbursement if not applied correctly. Telehealth anesthesia services, ICU procedures, and evolving anesthesia techniques have further increased the need for the timely adoption of updated coding standards. According to surveys, around 30% of anesthesia billing errors are linked to outdated or misapplied codes, making continuous education, real-time coding alerts, and up-to-date billing software essential for compliance and revenue protection.
-
Coordination with Multiple Insurance Payers
Anesthesia practices often deal with a variety of commercial and government payers, each with unique billing requirements, documentation expectations, and prior authorization rules. Misalignment between payer guidelines can result in claim denials or delayed payments. Effective coordination requires meticulous verification, submission accuracy, and proactive follow-up tasks that are time-consuming without specialized AR or billing support.
Common CPT Codes and Billing Units in Anesthesia
Anesthesia billing relies on precise documentation of CPT codes, billing units, and modifiers. Each code corresponds to a specific procedure, the complexity of care, and the duration of anesthesia services. Errors in coding, misapplied modifiers, or inaccurate time tracking can lead to claim denials, delayed reimbursements, and revenue loss. According to industry data, 12–18% of anesthesia claims are denied on first submission, and practices can lose up to 15% of annual anesthesia revenue due to coding or documentation errors. Understanding common CPT codes, their base and time units, reimbursement ranges, and potential pitfalls is critical for maximizing revenue and minimizing risk.
The table below provides a detailed overview of major anesthesia CPT codes used in 2024–2026, along with billing units, average reimbursement, denial risk, and revenue impact:
| CPT Code | Procedure / Description | Base Units | Time Units (Typical) | Common Modifiers | Average Reimbursement (USD) | Denial Risk | Revenue Impact Notes |
| 00126 | Ear procedures (biopsy, tympanotomy) | 2–4 | 2–3 (30–45 min) | AA, QK, QX, QY | $120–$250 | Moderate (10–12%) | Minor procedures; small errors in time or modifier can reduce reimbursement by $15–$25 per claim |
| 00626 | Thoracic spine / cord procedures (anterior approach, 1-lung ventilation) | 5–8 | 4–6 (60–90 min) | QK, QX, QY | $450–$750 | High (15%) | Medium-complexity procedures; accurate time documentation and modifier usage critical to avoid denials |
| 00326 | Pediatric larynx / trachea procedures (<1 year old) | 6–10 | 3–4 | AA, QK, QX | $400–$800 | High (18–20%) | High-risk pediatric cases; missed physical status modifiers or age misreporting can result in 10–15% revenue loss per claim |
| 01234 | Radical resections / major orthopedic surgeries (femur, long bones) | 12–19 | 8–12 (120–180 min) | AA, QK, QX, P3–P6 | $1,200–$2,500 | Very High (20%) | Complex procedures; small documentation errors can lead to $200–$500 lost per claim; physical status modifiers significantly affect total units |
| 00702 | Upper anterior abdominal wall procedures (e.g., percutaneous liver biopsy) | 4–6 | 2–3 | AA, QK, QX, QY | $300–$550 | Moderate (12–15%) | Accuracy in modifiers and patient status essential; errors can reduce reimbursement by $30–$50 |
Key Takeaways:
- Total Anesthesia Units = Base Units + Time Units + Modifiers (including Physical Status).
- Example: Thoracic spine procedure (Base 6 + Time 6 + QK + P2) → 13–14 total units, corresponding to $600–$700 reimbursement.
- Even small errors in CPT selection, time documentation, or modifier usage can cost practices thousands of dollars annually, highlighting the importance of meticulous billing practices.
- Regular audits, staff training, and automated anesthesia billing software can help reduce denials and maximize revenue recovery.
Benefits of Outsourcing Anesthesia Billing Services
Outsourcing anesthesia billing services helps practices improve accuracy, accelerate reimbursements, and reduce administrative burden. With anesthesia billing involving complex units, modifiers, and time tracking, specialized expertise can significantly enhance revenue cycle performance.
-
Increased Financial Accuracy and Faster Reimbursements
Anesthesia billing is highly specialized, involving base units, time units, modifiers, and physical status codes. Even minor coding errors can lead to denials or underpayments. Studies show that practices outsourcing anesthesia billing see up to a 25% reduction in claim denials and a 15–20% improvement in first-pass clean claim rates. Specialized billing teams ensure that documentation is accurate, units are properly calculated, and CPT codes are correctly applied, which helps practices receive payments 30–45 days faster on average compared to fully in-house billing.
-
Optimized Cash Flow and Revenue Recovery
Revenue leakage is a major concern in anesthesia services. Inefficient billing can lead to lost revenue ranging from 8–15% annually. Outsourced billing providers monitor claims continuously, identify high-risk accounts, and perform timely follow-ups on pending or denied claims. This proactive approach allows practices to recover a higher percentage of previously uncollected revenue and maintain predictable cash flow, a crucial factor for practice sustainability and growth.
-
Time and Resource Savings
Handling complex anesthesia billing in-house demands specialized training, meticulous documentation, and continuous monitoring of payer updates. Outsourcing shifts this administrative burden to experts, allowing anesthesiologists, CRNAs, and staff to focus on patient care. Surveys indicate that practices outsourcing billing report saving 10–15 hours per week per provider in administrative tasks, freeing staff to dedicate more time to clinical responsibilities and patient satisfaction initiatives.
-
Compliance and Regulatory Support
Anesthesia billing is subject to frequent updates in coding standards, payer rules, and regulatory guidelines. Outsourced billing companies stay up-to-date with CMS regulations, ASA updates, and payer-specific rules. This reduces the risk of compliance errors, audits, and potential penalties. Data from healthcare revenue cycle reports suggest that practices leveraging specialized billing services have 35–40% fewer compliance-related claim corrections compared to practices managing billing internally.
-
Scalability and Flexibility
Outsourced billing solutions can adapt to changes in patient volume, surgical case mix, or payer requirements. Whether a practice experiences seasonal fluctuations in surgical cases or expands into new procedures, external billing teams provide scalable support without the need for hiring and training additional in-house staff. This ensures consistent revenue cycle performance and operational efficiency, regardless of practice growth or complexity.
Outsourcing anesthesia billing improves accuracy, reduces denials, and strengthens cash flow. By combining expertise, compliance, and scalability, it allows practices to focus on patient care while maximizing revenue.
Emerging Trends Impacting Anesthesia Billing in 2026
Anesthesia billing in 2026 is undergoing rapid transformation driven by regulatory changes, payer behavior, and advanced technology adoption. Unlike traditional billing workflows, anesthesia revenue cycle management is now influenced by evolving reimbursement models, stricter compliance requirements, and increasing reliance on data analytics. These shifts are making anesthesia billing more complex and more strategic than ever before.
-
Declining Reimbursement and Conversion Factor Pressure
Anesthesia reimbursement continues to face downward pressure despite slight adjustments in conversion factors. The 2026 CMS Physician Fee Schedule reflects minimal increases that fail to offset rising operational costs, leading to tighter margins for anesthesia practices.
As a result, even small inefficiencies in billing, such as incorrect unit calculations or missed modifiers, can significantly impact overall revenue. Practices must now focus on optimizing every billing component to maintain financial stability.
-
Increased Audit Scrutiny and Compliance Requirements
Payers are using advanced analytics to monitor billing patterns, especially around medical direction, concurrency, and modifier usage. In 2026, audit scrutiny has intensified, with a strong focus on documentation accuracy and compliance.
Even minor inconsistencies in time reporting or missing attestation for medically directed cases can trigger audits or payment reductions. This shift makes compliance not just a requirement, but a critical revenue protection strategy.
-
Telehealth Integration and Changing Care Models
Telehealth policies introduced during previous years are now becoming a permanent part of healthcare delivery. The 2026 CMS updates integrate telehealth into routine workflows, affecting how anesthesia-related pre-op and post-op services are documented and billed.
While telehealth improves access and flexibility, it also introduces new billing rules, documentation standards, and payer-specific requirements that increase billing complexity.
-
Shift Toward Value-Based Care and Quality Reporting
The transition toward value-based care models, including participation in quality programs like MIPS, is impacting anesthesia billing. Providers now need to align billing practices with performance metrics and reporting requirements.
However, anesthesia practices often face challenges due to limited applicable quality measures, increasing the risk of penalties rather than incentives if reporting is not optimized.
-
Rising Administrative Complexity and Workflow Challenges
Billing workflows are becoming more complex due to evolving payer rules, multi-payer coordination, and documentation requirements. Administrative burden continues to rise without proportional increases in reimbursement.
This complexity increases the risk of delays, denials, and revenue leakage, especially for practices relying on manual processes or outdated systems.
-
Adoption of AI and Data-Driven RCM Solutions
Artificial intelligence and automation are reshaping anesthesia revenue cycle management. AI-driven tools can identify denial patterns, flag high-risk claims, and optimize workflows in real time.
Practices adopting these technologies gain a competitive advantage through faster reimbursements, reduced AR days, and improved financial visibility, while those relying solely on manual processes risk falling behind in an increasingly data-driven environment.
Why These Trends Matter
These emerging trends highlight a critical shift: anesthesia billing is no longer just about accurate coding; it is about strategic revenue optimization.
Practices that adapt to these changes by improving compliance, leveraging technology, and optimizing workflows will achieve:
- Faster reimbursements and reduced AR days
- Lower denial rates and audit risks
- Stronger, more predictable cash flow
In contrast, practices that fail to evolve risk increased denials, revenue leakage, and operational inefficiencies in an already high-pressure reimbursement environment.
Best Practices to Master Anesthesia Billing in 2026
Anesthesia billing is complex, but with the right systems and habits, errors can be minimized and revenue maximized. Here’s how top-performing practices stay ahead:
- Standardize Documentation: Use EMR-integrated templates to ensure every procedure is recorded accurately and consistently, from induction to emergence.
- Track Every Minute: Precise start, end, and emergence times are critical; every 5–10 minutes can impact reimbursement. Automated time-tracking tools help eliminate human error.
- Apply Modifiers Correctly: AA, QK, QX, QY, and physical status modifiers must reflect actual provider roles and patient complexity. Consistency here reduces denials and compliance risks.
- Stay Current with Guidelines: ASA standards, CPT updates, and payer-specific rules change frequently. Regularly update your coding knowledge and audit workflows to prevent revenue loss.
- Use Technology to Catch Errors: Denial alerts, real-time verification, and AI-driven billing checks catch mistakes before claims go out, saving time and protecting cash flow.
- Invest in Staff Training: Well-trained billing staff who understand anesthesia coding nuances are your first line of defense against errors and denials.
By combining technology, training, and standardized workflows, anesthesia practices can transform billing from a potential revenue drain into a predictable, high-performing financial engine.
The Role of Technology and AI in Anesthesia Billing
In 2026, technology isn’t just helpful; it’s essential for accurate anesthesia billing. AI and automation streamline complex workflows, reduce errors, and protect revenue. Modern tools can automatically check CPT codes and modifiers, flag high-risk claims with predictive denial analytics, and integrate seamlessly with EMRs to ensure precise time tracking.
The result? Faster reimbursements, fewer AR days, and clearer financial visibility. Practices that embrace AI consistently outperform those relying on manual processes, turning billing from a time-consuming task into a strategic advantage for revenue and compliance.
Why Choose Health Quest Billing for Your Anesthesia Revenue Cycle
Anesthesia billing in 2026 is complex, time-sensitive, and constantly evolving. Health Quest Billing takes this burden off your shoulders, ensuring your practice maximizes revenue while staying fully compliant. Our certified anesthesia billing and coding specialists handle every nuance from precise time units and modifiers to payer-specific rules, reducing denials and accelerating reimbursements.
We optimize your entire anesthesia revenue cycle, ensuring claims are submitted correctly the first time and denials are managed proactively. With Health Quest Billing, your practice benefits from improved cash flow, faster AR recovery, and more predictable financial performance, all while freeing your staff to focus on patient care.
Partnering with Health Quest Billing transforms anesthesia billing from a source of stress into a strategic advantage, helping your practice operate efficiently and securely in 2026.
Conclusion
Anesthesia billing is no longer just paperwork; it’s a strategic revenue driver. Every unit, modifier, and minute counts. Practices that stay updated, adopt best practices, and leverage expert RCM support enjoy faster reimbursements, lower denial rates, and stronger cash flow. Errors are costly, but with precise billing and proactive management, revenue is protected and practice growth is supported.
Partner with Health Quest Billing to simplify your anesthesia revenue cycle, maximize every claim, and focus on what matters most: your patients. Don’t leave revenue on the table; let us handle the complexities.