Your cardiology practice may be performing more procedures than ever, but when claims remain in accounts receivable (AR) for 60, 90, or even 120+ days, earned revenue gets delayed instead of reaching your practice. In cardiology, where high-value services such as cardiac catheterizations, electrophysiology (EP) procedures, pacemaker implantations, ICD placements, nuclear stress tests, and advanced cardiac imaging are routine, even small reimbursement delays can quickly accumulate into significant cash flow pressure.
In most cases, the challenge is not patient volume, coding accuracy, or claim submission—it begins after the claim reaches the payer. Authorization requirements, medical necessity reviews, documentation requests, and payer-specific rules often slow down reimbursement even for clean claims. As these claims age, they begin to impact cash flow, provider compensation, staffing stability, and growth planning. What starts as a delay in payment can quickly turn into a serious AR problem and ultimately a write-off risk. This is where effective cardiology accounts receivable management becomes essential for protecting revenue and maintaining financial stability.
What Is Cardiology Accounts Receivable Management?
Cardiology AR Management is the process of tracking, managing, and collecting payments owed for cardiology services after claims have been submitted to insurance payers. It involves monitoring unpaid claims, resolving denials, appealing underpayments, following up with payers, and ensuring timely reimbursement for services provided.
Because cardiology procedures often involve high reimbursement values and complex payer requirements, effective AR management plays a critical role in maintaining cash flow and financial stability. Strong cardiology AR management helps practices reduce aging receivables, improve collection rates, identify revenue leakage, and strengthen overall revenue cycle performance.
Why Cardiology AR Days Are Increasing in 2026
Many cardiology practices are experiencing longer reimbursement cycles than ever before. While billing accuracy remains important, the primary causes of rising AR days now occur after claim submission.
Increased Payer Scrutiny
Insurance carriers continue to apply additional review processes to high-cost cardiology services, including:
- Cardiac catheterizations
- Electrophysiology procedures
- Pacemaker implantations
- ICD placements
- Cardiac CT and MRI studies
Even clean claims may experience payment delays while payers perform utilization reviews and medical necessity validation.
Expanding Prior Authorization Requirements
Many advanced cardiology services require authorization before reimbursement can be approved.
Common issues include:
- Missing authorization numbers
- Expired approvals
- Incorrect authorization details
- Mismatched service dates
Authorization-related problems frequently result in delayed payments, denials, and increased AR aging.
Medicare Advantage Complexity
Medicare Advantage plans continue to create additional reimbursement challenges for cardiology practices.
Compared to Traditional Medicare, Medicare Advantage plans often require:
- Additional clinical documentation
- Plan-specific billing requirements
- Prior authorization verification
- Extended review periods
These factors contribute significantly to aging AR balances.
Telecardiology and Remote Monitoring Growth
The expansion of remote patient monitoring (RPM) and telecardiology services has introduced payer-specific billing requirements that vary widely among insurers.
Incorrect modifiers, documentation deficiencies, and place-of-service errors frequently delay reimbursement for remote monitoring claims.
Cardiology AR Aging Breakdown (Where Revenue Gets Stuck)
Cardiology AR aging shows how long unpaid claims remain in the revenue cycle before being collected or written off. In cardiology, each aging stage reflects increasing financial risk, with recovery becoming more difficult as claims age.
AR Aging Stages in Cardiology (2026)
| AR Aging Stage | Status | Revenue Impact | Action Required |
|---|---|---|---|
| 0–30 Days | Standard processing phase | Claims are under initial payer review and typically follow normal payment timelines | Monitor claim status and ensure clean submission |
| 30–60 Days | Early delay stage | Slower payer response begins; risk of processing delays increases | Start follow-ups and verify documentation completeness |
| 60–90 Days | High-risk / denial transition zone | Claims are at high risk of denial, rework, or documentation requests | Escalate follow-ups and initiate denial prevention actions |
| 90+ Days | Revenue leakage zone | Low probability of full recovery; increased chance of write-offs | Immediate escalation, appeals, and recovery prioritization |
Most cardiology revenue loss does not occur at the billing stage it happens after claims cross 60 days in AR, when delays begin converting into denials and recovery becomes significantly more difficult.
Common Cardiology Denials That Drive Up AR Days
In cardiology billing, denials are not isolated errors they are direct triggers of delayed cash flow and extended AR cycles. Even when claims are eventually paid, the recovery timeline often stretches into weeks or months, increasing AR pressure across the practice.
Below are the most common denial types impacting cardiology revenue in 2026:
1. Medical Necessity Denials
These denials go beyond documentation issues they directly slow down reimbursement and often push claims into 60–90+ day AR aging buckets.
They typically occur when payer reviewers determine that clinical documentation does not fully justify high-cost cardiology services such as advanced imaging, catheterization, or device implantation. In most cases, the issue is not a lack of service but a missing clinical narrative that connects symptoms, diagnostics, and treatment decisions clearly.
Extended payer reviews, delayed approvals, and increased risk of partial or full non-payment.
2. Modifier Errors
Incorrect or missing modifiers such as 26, TC, 59, RT/LT, and 25 remain one of the fastest causes of claim rejection or payment reduction in cardiology billing Many of these errors are automatically detected by payer systems before claims even reach manual review, causing instant delays in processing.
Immediate claim holds, reduced reimbursement, and avoidable rework cycles that slow down AR movement.
3. Authorization Denials
Authorization-related issues continue to be a major AR driver for cardiology practices, especially for high-cost procedures like imaging, EP studies, and cardiac interventions Missing, expired, or incorrectly submitted authorizations often result in claims being placed on hold or fully denied.
Claims enter long appeal cycles, significantly increasing AR backlog and delaying cash recovery.
4. Telehealth Compliance Denials
As telecardiology and remote monitoring continue to expand, payer-specific billing rules have become increasingly inconsistent.
Claims are frequently denied when:
- Incorrect POS codes are used
- Modifier 95 (or payer-specific equivalents) is missing
- Telehealth documentation does not meet interactive service
Even small formatting or documentation errors can trigger claim suspension or reprocessing delays. Unpredictable payment timelines, increased follow-up workload, and extended AR aging for telehealth-related services.
Medicare vs. Commercial Payers: AR Challenges in Cardiology
| Payer Type | AR Behavior | Key Challenges | Best AR Strategy |
| Traditional Medicare | Faster processing | Post-payment audits, recoupments | Audit-ready documentation |
| Medicare Advantage | Slower, inconsistent | Layered authorizations, policy variation | Plan-specific workflows |
| Commercial Payers | Highly variable | Utilization review, delayed approvals | Aggressive follow-up & segmentation |
Understanding payer behavior allows cardiology practices to prioritize follow-up strategically, reducing AR aging.
High-Impact AR Reduction Strategy for Cardiology Practices (2026)
Effective AR reduction in cardiology is not based on equal claim follow-up; it is based on a financial prioritization hierarchy, where claims are managed based on revenue value, payer behavior, and recovery probability.
1: High-Revenue, High-Risk Claims (Priority Recovery Layer)
Focus first on the highest financial impact procedures, including:
- Electrophysiology (EP) procedures
- Cardiac catheterizations
- Device implantations (pacemakers, ICDs, LVAD-related services)
These claims represent the largest revenue exposure and are most likely to enter extended AR cycles due to prior authorization and documentation complexity.
2: Diagnostic & Imaging-Heavy Claims (Delay Sensitivity Layer)
Includes:
- Cardiac MRI and CT imaging
- Nuclear stress testing
- Advanced echocardiography services
These claims are highly sensitive to payer review cycles and often experience extended processing delays due to medical necessity validation.
3: E/M and Routine Cardiology Services (Volume Layer)
Includes:
- outpatient cardiology visits
- follow-up consultations
- chronic care management services
While lower in individual value, these claims represent high-volume AR accumulation and require consistent workflow automation to prevent backlog formation.
Leading cardiology practices do not reduce AR by working harder they reduce AR by sequencing recovery efforts based on revenue intensity and payer behavior predictability.
Most Common Cardiology Procedures Creating High AR Balances
Certain cardiology services are more likely to experience reimbursement delays due to their complexity and reimbursement value.
-
Nuclear Stress Testing
Frequently delayed due to medical necessity reviews and additional documentation requests.
-
Cardiac CT & MRI
Often held because of authorization issues, expired approvals, or payer-specific coverage policies.
-
Pacemaker & ICD Implantations
High-dollar procedures that commonly trigger operative report reviews and clinical documentation requests.
-
Electrophysiology Procedures
Require extensive documentation and authorization validation, increasing reimbursement timelines.
Why AR Is Critical for Cardiology Practices in 2026
Accounts Receivable (AR) represents revenue already earned but not yet collected. In cardiology, this gap directly impacts financial performance because claims involve high-dollar, high-review procedures.
High AR days affect:
- Cash Flow Stability → delays in operational liquidity
- Provider Payments → slower compensation cycles
- Growth Investment → limits expansion and technology upgrades
- Operational Load → increases billing team workload and rework cycles
In large cardiology groups, even a small AR delay can translate into significant monthly revenue blockage.
How Claims Get “Stuck” in Cardiology AR Systems
In cardiology revenue cycles, claims rarely become stagnant by chance they get trapped due to predictable breakdown points within payer and internal workflows.
1. Payer Holds (External Delay Layer)
Claims are placed on hold when payers initiate additional review steps such as:
- medical necessity validation for high-cost procedures
- device or imaging utilization review
- pre-payment audit triggers
Result: Claims remain in “pending review” status even when clean and complete.
2. Missing Trigger Events (Documentation Gaps)
Claims fail to progress when required clinical or administrative triggers are absent, such as:
- missing operative notes or diagnostic linkage
- incomplete modifier alignment (26, 59, RT/LT, TC)
- absent or expired prior authorization updates
Result: Claims do not move from “submitted” to “adjudication.”
3. Workflow Breakpoints (Internal Process Failure)
Even after payer acceptance, claims stall due to internal AR breakdowns such as:
- delayed denial follow-up cycles
- unworked aging buckets beyond 30–60 days
- lack of escalation pathways for high-value cardiology claims
Result: Claims remain in AR aging without resolution and eventually transition into write-off risk zones.
Most cardiology AR leakage does not occur from denial itself it occurs when claims stop moving through these three systems simultaneously: payer processing, documentation triggers, and internal AR workflows.
DSO Impact in Cardiology AR Cycles
As cardiology AR ages beyond 60 days, Days Sales Outstanding (DSO) increases significantly, directly affecting cash flow predictability in cardiology practices. Higher DSO indicates slower conversion of earned revenue into collected revenue, which creates liquidity pressure, delays provider compensation cycles, and limits reinvestment in high-cost cardiac services such as imaging, EP labs, and device programs. In 2026, controlling AR aging is no longer just a billing priority it is a direct financial control mechanism for stabilizing cardiology practice revenue.
Key AR Metrics Every Cardiology Practice Must Track in 2026
Tracking AR is not just about balances; it’s about visibility and control. Here are the key metrics your cardiology practice must monitor:
- Average AR Days: Keep AR days between 30-45 days. Anything over 60 days signals inefficiencies in the revenue cycle.
- AR Aging Breakdown: Categorize AR into 0–30 days, 31–60 days, 61–90 days, and 90+ days. Prioritize high-value claims, especially those in the 90+ days bucket.
- Clean Claim Rate: Aim for 90%+ clean claims to reduce rework and speed reimbursement.
- Denial Rate by Payer: Track denials separately for Medicare, Medicare Advantage, and commercial payers.
- First-Pass Resolution Rate (FPRR): A higher FPRR means claims are paid without needing follow-up.
- Authorization-Related AR Percentage: This metric helps you track how much of your AR is tied to pending or expired authorizations.
- Patient Responsibility Collection Rate: With the rise of high-deductible health plans (HDHPs), managing patient balances upfront is essential.
From $420,000 in Aging AR to Faster Collections: A Cardiology AR Recovery Example
A growing cardiology group was facing increasing reimbursement delays, with more than $420,000 tied up in aging accounts receivable. The biggest contributors included unresolved nuclear stress test claims, authorization-related delays, and Medicare Advantage claims awaiting documentation review.
After identifying the root causes and prioritizing high-value claims, the practice recovered a substantial portion of aging AR while improving cash flow visibility and reducing future reimbursement delays.
Case Study: Cardiology AR Recovery Project
The Challenge
| Key Challenges Identified During AR Review | Impact on Practice |
|---|---|
| $420,000+ in outstanding Accounts Receivable | Significant amount of earned revenue remained uncollected |
| 28% of claims aged beyond 90 days | Increased write-off risk and cash flow disruption |
| Backlog of unpaid electrophysiology (EP) and cardiac imaging claims | High-value procedures remained unresolved |
| Authorization delays for nuclear stress tests and cardiac CT scans | Claims experienced extended reimbursement timelines |
| Multiple Medicare Advantage claims pending review | Slower payment cycles and increased AR days |
| Limited follow-up on aging high-dollar claims | Revenue recovery opportunities were being missed |
Result: The practice maintained strong patient volume, but a large portion of earned revenue was not converting into timely collections.
Our Findings
| Root Cause Identified | Observation |
| Pending payer reviews | Claims remained in review without active follow-up |
| Missing documentation requests | Required records had not been submitted or tracked |
| Authorization discrepancies | Approval details did not match submitted claims |
| Medical necessity reviews | High-cost procedures faced additional payer scrutiny |
| Unappealed underpayments | Reimbursement discrepancies remained unresolved |
| Aging high-value claims | Several procedure claims remained unpaid for 120+ days |
The Solution
| AR Recovery Strategy | Objective |
| Prioritized high-value aging claims | Accelerate recovery of the largest outstanding balances |
| Escalated unresolved Medicare Advantage claims | Reduce payment delays and improve claim resolution |
| Resolved authorization-related issues | Prevent avoidable denials and reimbursement holds |
| Submitted additional clinical documentation | Support medical necessity and payer review requirements |
| Appealed denied and underpaid claims | Recover lost revenue opportunities |
| Implemented weekly AR follow-up workflows | Improve accountability and reduce future aging AR |
The Outcome
Within a few months, the practice saw a significant reduction in aging receivables and improved visibility into its revenue cycle performance. Most importantly, claims that had been sitting unresolved for months were actively worked, allowing the practice to recover revenue that was at risk of becoming a write-off.
How HealthQuest Billing Reduces Cardiology AR Days in 2026
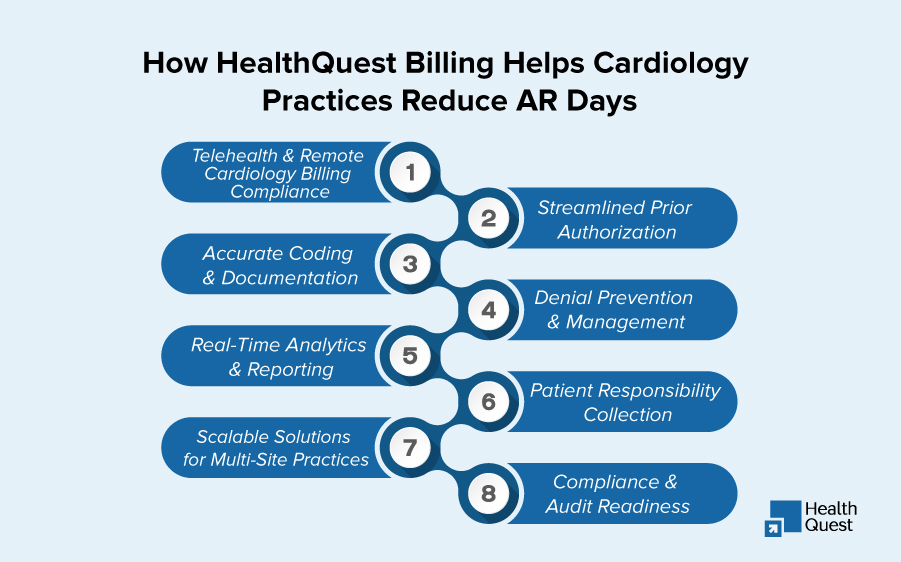
Conclusion:
Cardiology billing continues to grow more complex; relying on reactive AR management will only lead to delayed payments and rising write-offs. But with the right approach, tracking key metrics, addressing denial trends early, and aligning workflows with payer requirements, your practice can significantly reduce AR days even in today’s challenging reimbursement environment.
Don’t let AR cycles hinder your practice’s financial health. Partner with HealthQuest Billing today to protect your revenue, improve cash flow, and refocus on what truly matters: delivering exceptional patient care.