Anesthesia billing is one of the most modifier-dependent areas in healthcare revenue cycle management. Unlike many specialties where modifiers play a supporting role, anesthesia reimbursement is directly driven by accurate modifier selection, provider participation, medical direction compliance, and concurrency documentation.
In 2026, anesthesia practices are facing increased payer scrutiny around CRNA billing, concurrency rules, documentation requirements, and modifier usage. Even small inconsistencies can lead to denials, reduced reimbursement, audits, and long-term revenue leakage.
Because anesthesia services involve anesthesiologists, CRNAs, medical supervision rules, and time-based reimbursement structures, understanding modifiers is essential for maintaining clean claims and stable cash flow.
Why Anesthesia Modifiers Matter in Billing
Anesthesia modifiers do more than identify coding details; they directly determine reimbursement, provider responsibility, and compliance outcomes.
Payers use modifiers to evaluate:
- Whether anesthesia was personally performed
- Whether medical direction or supervision was involved
- How the concurrency rules were followed
- How payment should be split between providers
Unlike other specialties, anesthesia billing is highly dependent on CMS participation rules, concurrency management, and strict documentation standards. Even small inconsistencies can trigger underpayments, denials, or audits.
As payer scrutiny increases in 2026, modifier accuracy has become a core revenue cycle function, not just a coding task.
Anesthesia Modifier Mapping Table (Quick Reference)
This quick overview helps anesthesia practices understand how each modifier directly affects reimbursement structure, provider responsibility, and compliance risk in real-world billing scenarios.
| Modifier | Meaning | Key Risk Area | Common Denial Trigger |
| AA | Personally performed anesthesia | Documentation gaps | Missing continuous provider involvement |
| QK | Medical direction (2–4 cases) | Concurrency compliance | Exceeded or unverified concurrency |
| QY | Medical direction (1 CRNA) | Participation tracking | Weak attestation or missing records |
| QX | CRNA under medical direction | Documentation alignment | Missing linked physician claim |
| QZ | CRNA without medical direction | Payer variability | Non-covered supervision model |
| AD | Medical supervision (>4 cases) | Reimbursement reduction | Exceeded direction limits |
AA Modifier in Anesthesia Billing
The AA modifier is used when the anesthesiologist personally performs the entire anesthesia service without medical direction involvement from another provider.
This is generally considered the most straightforward anesthesia billing scenario because one provider manages the case from start to finish. However, documentation must clearly support complete provider involvement throughout the procedure.
Accurate AA billing typically requires:
- Complete anesthesia start and stop time documentation
- Pre-anesthesia evaluation
- Continuous provider participation
- Post-anesthesia assessment
Claims billed with AA can be denied if documentation indicates concurrent medical direction activity or CRNA participation that conflicts with personally performed anesthesia billing.
QK Modifier: Medical Direction of Multiple Cases
The QK modifier is used when an anesthesiologist medically directs two to four concurrent anesthesia procedures involving qualified providers such as CRNAs.
This modifier carries significant compliance risk because reimbursement depends on strict CMS medical direction requirements. The anesthesiologist must remain actively involved in the anesthesia care process while meeting all required participation standards.
Documentation must support:
- Pre-anesthesia evaluation
- Participation during induction
- Ongoing monitoring involvement
- Immediate availability during procedures
- Post-anesthesia participation
Incomplete attestations and concurrency violations are among the most common reasons QK claims fail audits or trigger payer recoupments.
QY Modifier in Anesthesia Billing
The QY modifier applies when an anesthesiologist medically directs one CRNA during a single anesthesia case.
Although QY involves only one concurrent procedure, payer expectations around documentation and medical direction remain strict. Providers must clearly document their participation and availability throughout the case.
Payers frequently review:
- Provider attestations
- Medical direction compliance
- Anesthesia time records
- Provider availability
- CRNA involvement
Because of rising payer scrutiny in 2026, many anesthesia groups now use internal concurrency tracking systems to reduce compliance exposure tied to QY billing.
QX Modifier: CRNA Services Under Medical Direction
The QX modifier identifies CRNA services performed under the medical direction of an anesthesiologist.
QX is commonly billed alongside physician modifiers such as QK or QY to reflect shared provider participation in the anesthesia service. Claims are often denied when the documentation between the physician and CRNA does not align correctly.
Most modifier-related QX denials happen because of:
- Missing physician modifiers
- Incomplete medical direction documentation
- Concurrency inconsistencies
- Provider assignment errors
Strong documentation workflows are essential for ensuring both CRNA and physician claims remain properly connected.
QZ Modifier in Anesthesia Billing
The QZ modifier is used when a CRNA performs anesthesia services without medical direction from an anesthesiologist.
As staffing shortages continue affecting healthcare systems, QZ billing has become increasingly common across hospitals, surgery centers, and independent anesthesia models. However, reimbursement rules for QZ vary significantly depending on payer contracts and state regulations.
Practices using QZ billing should carefully monitor:
- State supervision requirements
- Commercial payer policies
- Facility credentialing rules
- CRNA enrollment status
Incorrect QZ billing can create major reimbursement and compliance problems if payer-specific rules are not followed carefully.
AD Modifier and Medical Supervision Rules
The AD modifier applies when an anesthesiologist medically supervises more than four concurrent anesthesia procedures. Unlike medical direction billing, medical supervision generally reimburses at lower rates because the anesthesiologist cannot fully satisfy all CMS participation requirements across multiple overlapping cases.
This distinction has major financial implications for anesthesia groups managing high surgical volumes. Many practices unintentionally lose revenue when concurrency exceeds allowable medical direction limits without adjusting billing appropriately.
As operating room schedules become increasingly complex in 2026, active concurrency tracking has become a critical component of anesthesia revenue cycle management. Practices that fail to monitor supervision thresholds carefully often experience recurring underpayments, compliance risks, and audit exposure tied to incorrect modifier usage.
Medical Direction vs Medical Supervision in Anesthesia Billing
Understanding the difference between medical direction and medical supervision is critical for compliant anesthesia reimbursement. Payers treat both models differently, and even small documentation gaps can lead to reduced payments or audit risk.
Medical direction requires active anesthesiologist involvement throughout the case, including oversight, participation in key anesthesia activities, and maintaining required concurrency limits. Medical supervision applies when concurrency exceeds allowable thresholds or when documentation does not fully support medical direction criteria.
The financial impact is significant. Medical direction typically follows higher reimbursement rules, while supervision often results in reduced payment and increased audit exposure.
| Aspect | Medical Direction | Medical Supervision |
| Concurrency | Within CMS limits | Exceeds limits |
| Involvement | Active participation | Limited oversight |
| Reimbursement | Higher, structured payment | Lower reimbursement |
| Audit risk | Moderate | Higher |
Common Anesthesia Modifier Billing Mistakes
Most anesthesia modifier denials don’t come from major coding failures. They originate from small, repetitive workflow gaps that slowly compound over time. In many anesthesia practices, these issues often go unnoticed until denial rates rise, reimbursements slow, or A/R aging extends beyond normal cycles.
What makes modifier-related errors especially damaging is their direct impact on reimbursement methodology. Even a single mismatch in documentation or coding logic can shift a claim from full payment to reduced reimbursement or a complete denial. Over time, this creates hidden revenue leakage that is difficult to detect without structured auditing.
The most common anesthesia modifier issues include:
- Incorrect modifier combinations that don’t align with payer rules
- Missing physician attestations supporting medical direction or supervision
- Concurrency violations across multiple anesthesia cases
- Incomplete or inconsistent CRNA documentation
- Inappropriate use of AA modifier during medically directed cases
- Anesthesia time record inconsistencies (start/stop mismatches)
- Lack of standardized provider workflows across facilities
These issues are often systemic rather than isolated. That’s why they tend to repeat until a formal QA and modifier validation process is implemented across the revenue cycle.
Documentation Requirements for Anesthesia Modifier Compliance
Strong documentation is essential for accurate anesthesia modifier billing. Payers now require clear evidence of provider role, medical direction compliance, concurrency, and precise anesthesia timing. Without complete records, even correctly coded claims can be denied or flagged in audits.
A compliant anesthesia record should clearly support the modifier billed and include key clinical and billing elements.
Minimum required documentation:
- Provider participation throughout the case
- Accurate anesthesia start and stop times
- Pre-anesthesia evaluation
- Medical direction details (if applicable)
- Post-anesthesia assessment
- Transfer-of-care notes
Missing or inconsistent documentation commonly leads to denials, downcoding, and post-payment audits. Standardized templates help improve accuracy, reduce errors, and strengthen audit defense.
How Anesthesia Modifiers Impact Reimbursement (2026 Guide)
Anesthesia modifiers directly control how anesthesia services are priced and reimbursed by defining provider role, supervision structure, and compliance level. Because anesthesia billing is entirely modifier-driven, even minor inaccuracies can change payment outcomes or trigger denials.
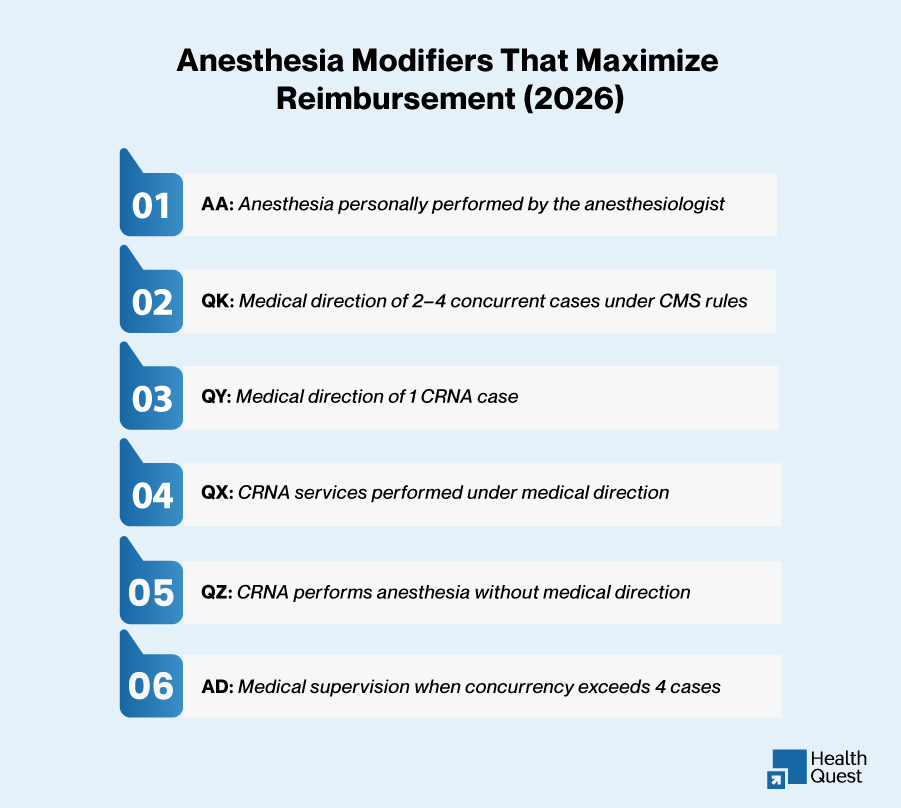
Each modifier represents a specific reimbursement model. AA applies to personally performed cases and reimburses the anesthesiologist based on base units and time. QK and QY reflect medical direction scenarios where payment is split between anesthesiologist and CRNA under CMS concurrency rules. QX identifies CRNA services under medical direction, requiring aligned documentation with the supervising physician. QZ applies to CRNA-only services, while AD indicates medical supervision when concurrency exceeds allowable limits, often reducing reimbursement due to compliance restrictions.
Common reimbursement impact issues:
- Payment variation due to incorrect model selection
- Split-payment errors between physician and CRNA claims
- Denials from mismatched or incomplete documentation
- Concurrency-related compliance discrepancies
- Differences in payer interpretation of CMS rules
Regular audit of modifier patterns and payer-specific rules is essential to prevent revenue leakage and maintain consistent reimbursement accuracy.
Anesthesia Billing Compliance Risks in 2026
Compliance risk remains one of the biggest challenges facing anesthesia groups today. Payers and government programs are under increasing scrutiny around:
- Concurrency violations
- Modifier misuse
- Missing attestations
- Improper CRNA billing
- Time inflation
- Provider participation inconsistencies
Practices that fail to monitor these areas carefully may face payment recoupments, audits, or long-term reimbursement instability.
Regular internal coding audits and documentation reviews help anesthesia groups identify compliance risks before payer investigations occur.
Best Practices to Reduce Anesthesia Modifier-Related Denials
Reducing anesthesia modifier denials requires proactive control, not reactive correction. Most issues start early due to documentation gaps, coding inconsistencies, or missed payer rules, making prevention more effective than denial management.
Key strategies:
- Pre-submission documentation validation
- Real-time concurrency monitoring
- Modifier checks aligned with payer rules
- Enforcement of billing and compliance standards
- Structured QA for high-risk cases
Strong coordination between providers, coders, and billing teams is also essential, as most errors stem from documentation misalignment rather than lack of coding knowledge.
Practices that apply these controls consistently see fewer denials, faster payments, and improved clean-claim performance.
The Role of Technology in Anesthesia Billing Accuracy
Technology has become a critical component of modern anesthesia billing, particularly in managing modifier complexity and concurrency tracking. As billing rules become more detailed, manual processes are no longer sufficient to maintain accuracy at scale.
Advanced anesthesia revenue cycle systems now help practices validate modifier combinations, track overlapping anesthesia cases, detect documentation gaps, and identify payer-specific billing rules before claims are submitted. This significantly reduces downstream denials and improves first-pass claim acceptance rates.
In addition, AI-driven analytics are transforming how anesthesia groups identify recurring billing issues. Instead of reviewing denials after they occur, practices can now detect patterns in real time, such as repeated modifier mismatches, documentation inconsistencies, or provider-specific billing errors.
This shift from reactive to predictive revenue cycle management is becoming a key differentiator for high-performing anesthesia organizations.
When to Outsource Anesthesia Billing Services
Many anesthesia groups choose to outsource billing because modifier management, concurrency tracking, and compliance monitoring require deep specialization and continuous oversight. These functions are difficult to maintain internally without dedicated expertise and advanced billing infrastructure.
A strong anesthesia billing partner should provide certified anesthesia coding expertise, real-time concurrency monitoring, denial management systems, payer-specific modifier analysis, credentialing and enrollment oversight, and audit-ready documentation workflows.
Outsourcing is not just about operational efficiency. It is about reducing compliance risk, improving reimbursement predictability, and ensuring long-term revenue cycle stability in an increasingly complex payer environment.
How HealthQuest Billing Supports Anesthesia Practices
HealthQuest Billing supports anesthesia groups by strengthening reimbursement accuracy through structured modifier-focused coding reviews, medical direction compliance monitoring, concurrency tracking systems, denial prevention workflows, and payer-specific billing analysis.
By combining deep anesthesia coding expertise with disciplined revenue cycle management processes, practices can reduce modifier-related denials, improve clean-claim performance, and achieve more stable and predictable financial outcomes over time.
Conclusion
Anesthesia modifiers directly control reimbursement accuracy, compliance, and cash flow. In 2026, payer scrutiny around concurrency, medical direction, CRNA billing, and documentation continues to increase, making modifier precision non-negotiable.
Most anesthesia denials are preventable and driven by workflow gaps, not coding complexity, leading to lost revenue, delays, and audit exposure when left unchecked.
Strong performance comes from disciplined documentation, strict modifier validation, and real-time concurrency control.